
Sleep apnea is a condition in which a person stops breathing while asleep. With sleep apnea, breathing while asleep is interrupted by repeated pauses known as apneic events. The types of sleep apnea include:
Recent investigations suggest that the severity of oxygen desaturation may be a stronger correlate with cardiovascular problems than the actual number of breathing interruptions. dThe drop in oxygen appears to unleash a whole host of changes, including release of catecholamines and inflammatory cytokines, which may play a role in injury and imperfect repair of blood vessels. Patients with sleep apnea have been shown to have a higher incidence and in most cases, sleep apnea treatment has been associated with decreased risk or clinical improvement. As for the impact on the eye? Yo-yo-ing oxygen levels have untold effects over the long term.
Sleep apnea can cause serious health problems. It can increase the risk for stroke, obesity, diabetes, heart attack/failure, high blood pressure, and more. Sleep apnea can also cause eye complications such as floppy eyelid syndrome, glaucoma, papilledema, retinal vein occlusion, and non-arteritic anterior ischemic optic neuropathy.
Snoring is almost always caused by a restricted airflow at the back of the throat. This happens when the jaw (and attached tongue, which is much larger than just the part we see) falls to the back of the mouth, so air has to be forced between the tongue and the back of the throat. This makes the throat vibrate loudly – causing snoring. Snoring happens when asleep because the jaw muscles go slack, so the jaw (and the attached tongue) fall back, narrowing the airway. This effect is made worse by lying on your back, causing the jaw to fall back more. Snoring is also worse when overweight, or relaxed after a drink or two.
The most common obstructive sleep apnea warning signs include:
If you share a bed with someone, they’ll probably notice it before you do.
It’s more likely if you’re overweight or obese, have a thick or large neck, or have smaller airways in your nose, throat, or mouth. It can also happen if you have enlarged tonsils or too much tissue at the back of the throat — the uvula and soft palate — that hangs down and blocks the windpipe. A larger-than-average tongue can also block the airway in many people as well as a deviated septum in the nose.
OSA is more common among men than women, and it becomes more likely as you get older. But it’s not a normal part of aging. Other risk factors include:
Just as it’s important for ophthalmologists to be alert to hypertension or mild diabetic retinopathy, it’s also critical to recognize visual conditions that might be associated with sleep apnea.
Floppy eyelid syndrome: One theory to explain floppy eyelid syndrome is a weak tarsal plate, common in obese patients; another involves the central nervous system. Normally, a person would be awakened by the sensation of pressure from pillows or bedding on an open eye, but “in patients with sleep apnea, a decrease in cortical arousability causes the eyelid to remain open when disturbed by mechanical stress during sleep,” he said. Over time, the lid becomes more lax and is easily everted with slight lateral traction.
Dr. Grover recommends referring patients with signs of lid laxity, especially men with other OSA risk factors, for a possible sleep study—even before full-blown signs of floppy eyelid syndrome appear. Topical treatment may help prevent papillary conjunctivitis and minimize symptoms such as dry eye, burning, and irritation.
Nonarteritic anterior ischemic optic neuropathy (NAION): in several large studies, 70 to 80 percent of patients with NAION have been found to have OSA. What originally prompted investigation into the links between NAION and sleep apnea is the classic presentation of acute painless vision loss upon awakening in the morning in 75 percent of NAION patients. Although it is not possible to reverse vision loss from NAION, he said, treatment for sleep apnea may help prevent an attack of NAION in the other eye, which occurs in 15 to 18 percent of cases.
Papilledema: Linked to idiopathic intracranial hypertension (IIH), which occurs most frequently in young women, papilledema may be associated with increased venous blood flow, said Dr. Golnik. An increase in CO2 concentration may result from interrupted breathing, he said, and it may dilate blood vessels and increase pressure, leading to optic disc swelling.
Dr. Golnik advocates questioning all papilledema patients about symptoms of sleep apnea. He sends patients who report symptoms for a sleep study, as well as those who don’t fit the usual IIH demographic, such as men or anyone over age 50. Dr. Golnik recently referred an IIH patient for evaluation and treatment, which improved her vision and papilledema within a matter of weeks. The sleep doctor was incredulous, asking, “How did you know? She had some of the worst apnea I’ve ever seen. You saved her life.”
Glaucoma. A number of studies have examined the possible connections between OSA and glaucoma, but they have yielded varying results. For example, a large chart review of 156,336 patients with a diagnosis of sleep apnea initially showed an increased risk of open-angle glaucoma (OAG), but the difference disappeared with multivariable analysis that accounted for confounding factors.2 In contrast, other researchers have shown associations, including a 2012 study that found a link not only to primary OAG but also to ocular hypertension. Glaucoma patients with OSA had a higher intraocular pressure (IOP), worse visual field indices, and thinner retinal nerve fiber layer compared with the control group.3
Retinal conditions. Studies suggest a causal relationship between central serous chorioretinopathy (CSCR) and OSA, said Dr. Grover, because of the known increase in catecholamines with OSA. “Although CSCR can resolve within six months of [ophthalmic] treatment, sleep apnea treatment in patients with the condition has been shown to accelerate the recovery,” he said, citing a case of bilateral CSCR in which the patient’s vision returned to 20/20 and 20/25 and the serous detachment resolved within a week of starting apnea treatment. Causing severe dysfunction in the autoregulation of three major blood vessels—the posterior ciliary, central retinal, and ophthalmic arteries—OSA-related hypoxia may be a culprit in retinal vein occlusions, said Dr. Grover. Hypoxia is also the primary stimulus for neovascularization in diabetic retinopathy, he said.5 In addition, OSA’s potential role in diabetic retinopathy was spotlighted in a recent Oxford study, which found a high prevalence of sleep apnea in patients with diabetic clinically significant macular edema (CSME). “When your retina doesn’t get enough oxygen,” said Dr. Holekamp, “this adds insult to injury, exacerbating existing underlying problems like diabetic retinopathy or hypertensive retinopathy. The tip-off is six or more peripapillary cotton-wool spots. Clinicians traditionally call this hypertensive retinopathy, but it may be a manifestation of blood pressure spikes from obstructive sleep apnea. Nothing is 100 percent, but I’m batting a thousand with the diabetic patients with cotton-wool spots I’ve referred for sleep studies.”
Your doctor will give you a checkup and ask about your sleep. He may also want to ask people who live with you about your sleep habits.
You may need to spend a night in a sleep lab or have a sleep study done at your house. You’ll wear monitors to measure things such as:
The study will track how many times your breathing was impaired during sleep.
For proper diagnosis of Obstructive Sleep Apnea (OSA) or other forms of sleep disordered breathing an overnight sleep test is necessary. The test consists of placing sensors on the body to measure certain body functions such as breathing, blood oxygen saturation, respiratory effort, body position, and brain activity. Different types of sleep tests use different sensors (also called channels) and the methods for obtaining sleep information differ slightly between tests.
Traditionally sleep tests have been conducted by an attended study in a sleep facility, rather than in the patient’s home. These attended studies are called Polysomnographs (PSG) and have been used for many years for the diagnosis of sleep disorder breathing, Obstructive Sleep Apnea, and other sleeping disorders. Recently home testing has become approved by the American Academy of Sleep Medicine for diagnosis of Obstructive Sleep Apnea. There is much debate in the medical community about which type of test is the most preferable, and below we discuss each type of test and the advantages and disadvantages of each:
Polysomnograph (PSG)
Home Sleep Test (HST)
The decision on which type of testing should be used for a particular patient can sometimes be a controversial issue in the medical community. One type of testing may not be appropriate for everyone. Someone who has symptoms of Obstructive Sleep Apnea (OSA) but has no other medical or sleep concerns may be accurately diagnosed with a Home Sleep Test (HST), while someone with a complicated medical and sleep history may be better suited to be test with a full Polysomnograph (PSG). Along with your physician, your Dental Sleep Solutions® dentist can help you determine which test might is best for your particular situation.
In 2009 the American Academy of Sleep Medicine (the foremost clinical group for health issues related to sleep) approved the usage of portable sleep testing for diagnosis of Obstructive Sleep Apnea (OSA) and other forms of sleep disorder breathing. According to the new clinical guideline, home sleep testing must be performed with a Level III portable sleep device that is is capable of measuring at least four different systems on the patient. The Home Sleep Test (HST) may be given to the patient by a trained technician, but diagnosis and interpretation of the results of the test must be made by a board-certified sleep physician. After instructions are given to the patient on how to attach the device, the patient takes the device home and wears it in their own home overnight. The device is returned to the sleep specialist who then interprets the results and gives a diagnosis. The home sleep recorders utilized by Dental Sleep Solutions® dentists are all clinically approved for home use, and diagnostic tests are evaluated by board-certified sleep physician.
iPhone Apps: There are some smartphone apps to record the snoring during sleep. These are a very limited measurement compared to the regular sleep studies, the PSG, and should not be used as a replacement for it. The Snoring Management App Record, measure and track your snoring and gives you the snoring intensity (Snore Score), Records sound samples, Tests the effectiveness of snoring remedies, and Tracks the impact of lifestyle factors.
Treatment options may include:
Store bought vs professionally fitted
It has become a regular occurrence for a reader to ask me “What’s the difference between online over-the-counter oral appliances and those fitted by a dentist?”. After receiving numerous request, I decided that it is time to address this question. While there are quite a few similarities between the two, they also differ in several ways. I am about to lay it out, the “straight dope” if you will, by examining these similarities and differences while comparing the two.
Lets start with the most important difference between a doctor fitted MAD and one purchased online. Several, but not all, OTC mouthpieces use simple boil and bite technology. They are fitted at home, typically using a pot of hot water. The molding process is fairly simple and involves heating the unit for a specified number of seconds in hot water and then placing it into the mouth. You then suck in, while pushing on the outside of your mouth to create a mold. After a few seconds the device is then dropped into a bowl of cold water which causes it to retain its shape.
There are of course some exceptions to this. For instance the SleepPro Custom and the Prosnore II both use a dental impression kit which the consumer uses to create an impression and then sends it off to a laboratory who then creates the mouthpiece which is then delivered directly to the consumer.
In comparison, professionally fitted oral appliances are sometimes boil and bite but are often created in a laboratory using an impression of your teeth. Your dentist will use dental trays to create a custom impression and then send this off to a lab to create a piece that closely hugs your teeth and gums. Once the device is returned from the lab, the dentist ensures a proper fit and makes adjustments if necessary.
In order to effectively control snoring, an oral appliance must be adjustable. Small incremental adjustments, typically 1 mm at a time, slowly pulls the jaw forward to the “advanced position”. By advancing the jaw too much at once, one can expect extreme facial tenderness in the morning. The idea is to advance the jaw forward into somewhat of a comfortable position while effectively reducing or eliminating snoring. This is often accomplished by adjusting the settings a couple millimeters at a time. Some OTC devices offer this while others do not. Almost all professionally fitted devices should feature some type of adjustment.
Generally speaking, professionally fitted oral appliances tend to have a longer useful life. The amount of time in which the appliance lasts will vary depending upon manufacturer. For the most part, pro fitted devices will last anywhere from a couple years to five years. This estimate will greatly vary depending on factors such as how often it is used (hopefully every night) and whether or not you grind your teeth at night (bruxism).
Over the counter devices have a typical useful life of anywhere from 3 months to 24 months. On average they last about a year or so, once again depending on several factors.
Cost
Perhaps one of the most notable difference between doctor fitted snoring mouthpieces and those ordered online is obviously the price. Over the counter devices will cost anywhere from $35 up to $200.
Going the professional route, one can expect to pay $300 – $500 for the initial examination and consultation in addition to the cost of the device of your choice which typically runs between $1,200 and $2,000. After the initial fitting you will be advised to return for adjustments. These appointments will typically cost $100 or more per visit. During the first 6 months you will likely return 2-3 times and thereafter you will be scheduled for a annual or bi-annual checkup. Keep in mind that you may be able to offset these costs depending on your insurance coverage, if available.
Do-it-yourself oral appliances are often criticized by medical professionals for a number of reasons. While some speak out over concerns for patients safety, others are unwelcoming of such OTC devices due to obvious monetary losses.
In May of 2012 Dr. Lydia Sosenko, a seller of oral appliances, featured Dr. Gail Demko in a podcast which was posted on Dr. Sesenko’s website. Dr Demko is considered to be an expert in the field of sleep apnea.
During the podcast Dr. Demko was asked “What is the biggest difference between professional devices and over the counter devices?” (@25:00 mins) Her response:
“There is a dentist that is watching the patients for side effects. Custom fitted devices fit snugly on the teeth and don’t loosen up in the mouth. They don’t fall out and end up in the bed two or three times a night. They are easy for the patient to adjust, they are not just one piece. They are comfortable and don’t cut into the gums. They don’t torque the teeth. They put pressure on all of the teeth instead of just one. And they are not put in the mouth of a patient whose not a good candidate.”
Dr. Demko brings up at least two valid point. With an over-the-counter device there is not a dentist watching the patient for side effects and they are not put into the mouth of a patient who may not be a good fit. As for the other 6 reasons cited, these can be debated and are not necessarily true with every DYI mouthguard.
OTC snoring mouthpieces should not be used to treat undiagnosed cases of Obstructive Sleep Apnea (OSA). If you suspect that you have sleep apnea or any other sleep disorder, it is essential to consult with your doctor who will likely suggest that you have a sleep study conducted.
If you are have conditions such as TMJ, gum disease, loose teeth, etc. you should consult with your dentist before using any oral appliances.
Now to answer the question: Which one is better? Obviously you can not go wrong with a professionally fitted oral appliance but if the price tag is preventing you from purchasing one, there are some really great snoring mouthpiece alternatives that can be ordered online. Here are a few key characteristics that I find desirable when purchasing such a device:
If you choose an over the counter device aim for one that has several of the above mentioned attributes and is within your price range. There are literally dozens of affordable products available on the market that can help with simple snoring. Here is a comparison chart that features several of them. Remember, when in doubt, have the doctor check it out!
The SleepTight Mouthpiece was designed by Dr. Michael Williams and is one of the few inexpensive MAD’s that has been cleared by the Food and Drug Administration for the treatment of snoring and mild to moderate obstructive sleep apnea in adults. Very few economy mouthpiece manufacturers are able to make this claim. Its dual laminate design ensures a tight fit that will last up to 24 months. The SleepTight can be purchased online for a fraction of the cost charged by most dentists and can be fitted at home in only a few minutes. Here are a few key points to consider:
Posted by Kevin Phillips
People do not wake up one morning suddenly afflicted with obstructive sleep apnea. Rather, obstructive sleep apnea (OSA) is believed to be a progressive disorder that lies on the extreme end of a spectrum of sleep disordered breathing.
At the other end of the spectrum is benign snoring–snoring that has no impact on sleep health other than possibly disrupting one’s bed partner’s sleep. When the causes of snoring begin to progress from relatively harmless noise-making to the harmful sleep disorder of sleep apnea, it often first develops into upper airway resistance syndrome (UARS).
But what exactly is UARS? How does it differ from OSA? And what treatments are available to keep it from developing into OSA? Here we hope to answer these questions and more.
First we will need a brief recap of what snoring is, as UARS is a progression towards OSA from snoring.
Snoring is the sound created when air flows past loose or relaxed tissues in the throat, which causes the tissues to vibrate and thus creates an irritating sound.
Snoring is an indication that some type of resistance is occurring in the upper respiratory system. The greater the resistance, the greater the breathing effort needed to get past the resistance.
Upper airway resistance syndrome occurs when that breathing effort crosses over from just being harmless snoring to a possibly troublesome disorder.
Causes of UARS are similar to OSA. It can be caused by a naturally narrowed air passage, loose fatty tissues of the throat collapsing back into the airway, or the position of the tongue (falling back) during sleep.
Patients with UARS require a greater effort in breathing to get past obstructions. Not all patients with UARS snore, and their symptoms may sound more like heavy, labored breathing during sleep. Sufferers of UARS often describe their breathing effort as “trying to breathe through a straw.”
Similar to OSA, the brain has to arouse itself from deeper stages of sleep to increase respiratory effort. When the brain is constantly being aroused from the deeper stages of sleep, it’s not able to perform other important tasks that it needs to complete so that you can feel refreshed in the morning. This can lead to symptoms of chronic fatigue and excessive daytime sleepiness, which are also present in obstructive sleep apnea.
Patients can move from snoring to UARS as a result of aging (as muscle tone decreases in the throat) and weight gain (increase of fatty tissues in the throat, which can increase material resistant to airflow). Women in their third trimester of pregnancy are also more likely to develop UARS as a result of weight gain.
One of the key differences between upper airway resistance syndrome and obstructive sleep apnea is that apneas (pauses in breathing) and hypopneas (decreases in breathing) are either absent or very low in patients with UARS.
Patients with OSA are often overweight or obese (although they can be of normal weight), whereas patients with UARS are often of average weight.
OSA is twice as likely to affect men as women, while UARS can affect men and women equally.
Obstructive sleep apnea is related to many more long-term health conditions as a result of apneas and hypopneas due to the decrease in blood pressure during apnea/hypopnea events, which can lead to increased risk of high blood pressure, heart disease, heart arrhythmias, stroke, and heart failure.
Patients who fail to treat UARS can end up developing OSA and find themselves at risk for many of these health problems.
Treatments for UARS are often similar to the treatments of OSA. However, CPAP therapy may be a last resort treatment option for UARS, rather than the “go-to” treatment that it is for OSA.
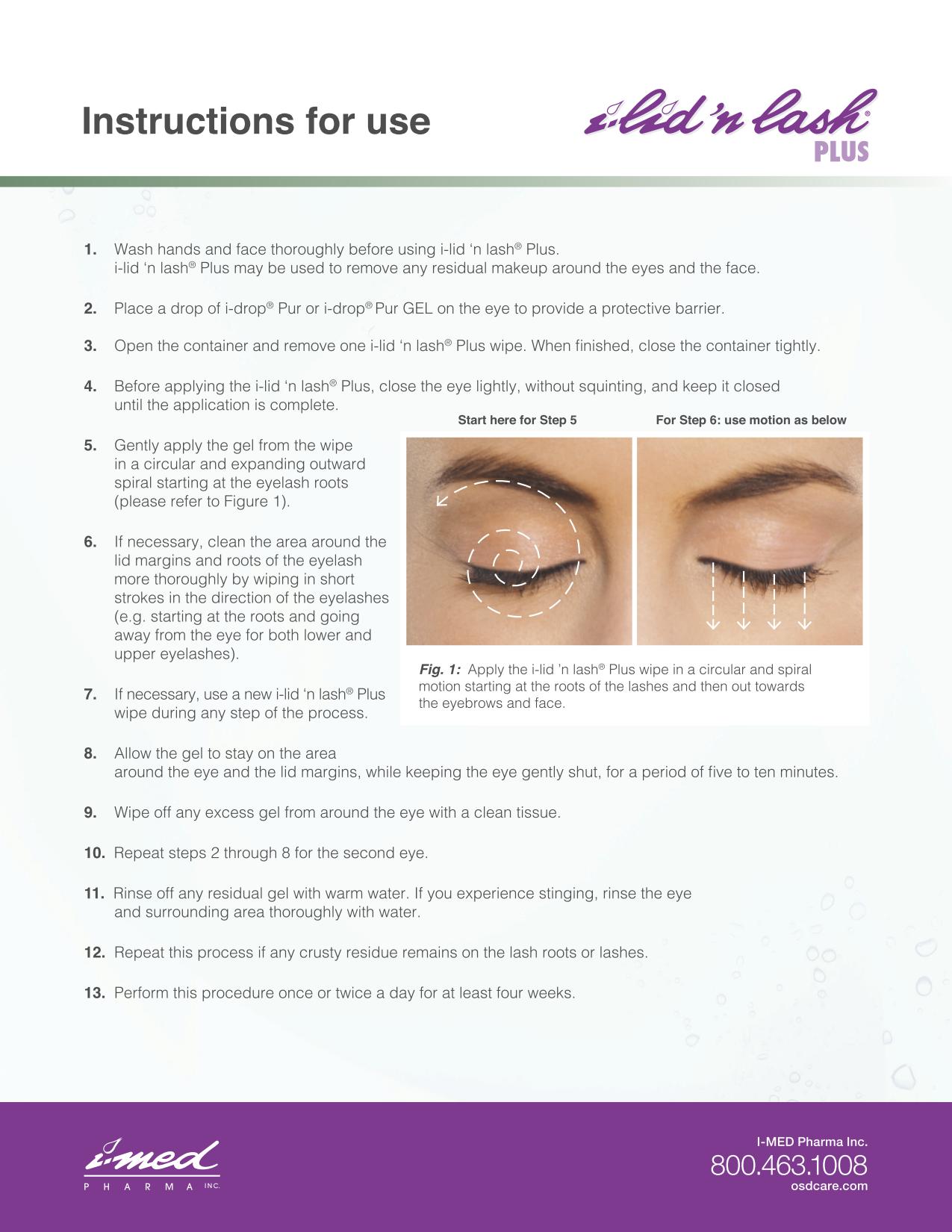
We recommend using special lid wipes formulated with 5% tea tree oil such as the I-LID ‘N LASH® PLUS (can be purchased at PVSC). Lids and lashes should be cleaned every night before going to bed. Make sure you are wiping vigorously to get the oil into the lash roots and along the lashes to kill any eggs. For instructions on how to use, click here.
If the I-LID ‘N LASH® PLUS is not working with consistent use, at PVSC we can perform a professional cleanup using the I-LID ‘N LASH® PRO (20% tea tree oil for professional use only) and the BlephClean.
Patients must also institute an eye hygiene regimen at home.
{kind=link}