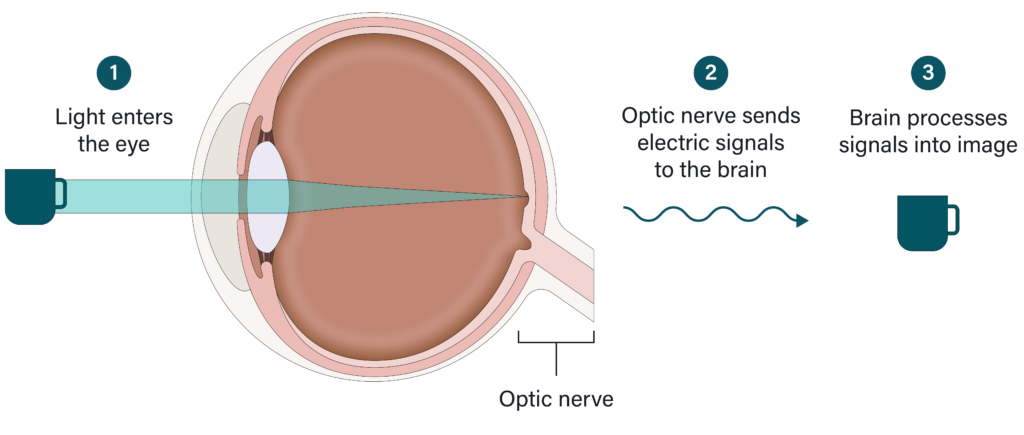
High eye pressure alone doesn’t cause glaucoma but it is a significant risk factor.
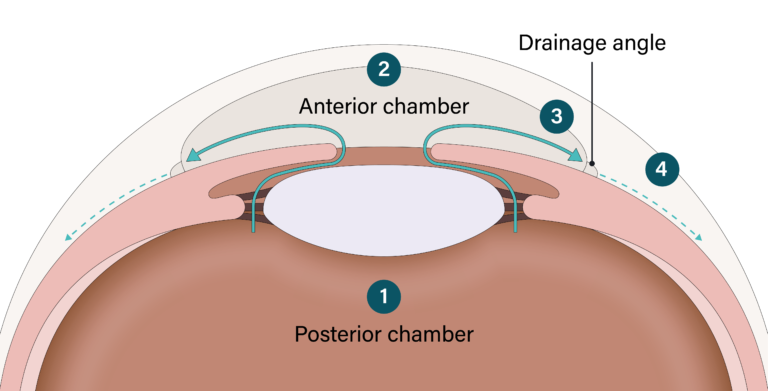
Your eye produces a clear liquid called aqueous humor. Its job is to circulate around the front part of the eye providing nutrients and giving it its shape. In a healthy eye, aqueous humor is constantly produced in small amounts at a time while equal amounts flow out. This is how your eye makes sure the pressure inside stays balanced.
Aqueous humor is produced in the back of the eye (posterior chamber) (1) then flows through the pupil into the front of the eye (anterior chamber) (2). It then flows out through a structure called the drainage angle (3) and drains into the eye’s circulatory system (4).
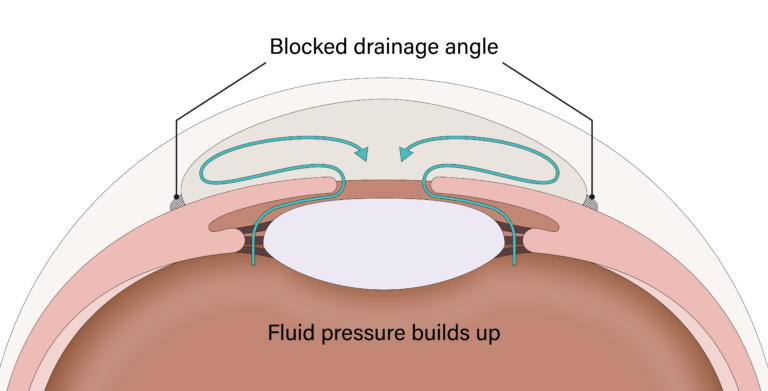
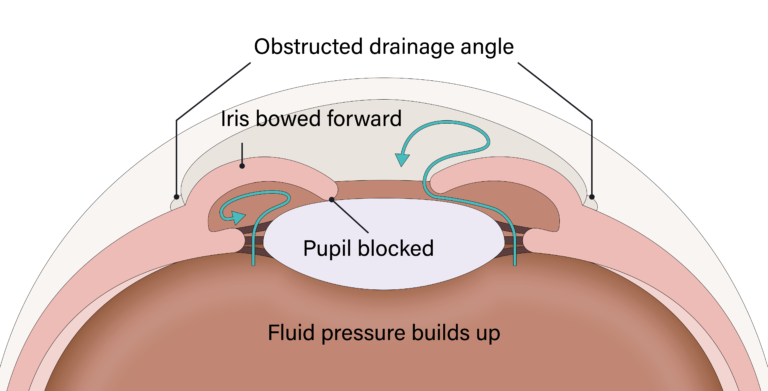
If the aqueous humor isn’t able to flow out properly, this can cause the pressure to rise higher than normal (think of a blocked garden hose). Fluid pressure builds up and causes damage to the blood vessels and optic nerve over time. If left untreated, this can cause blindness.